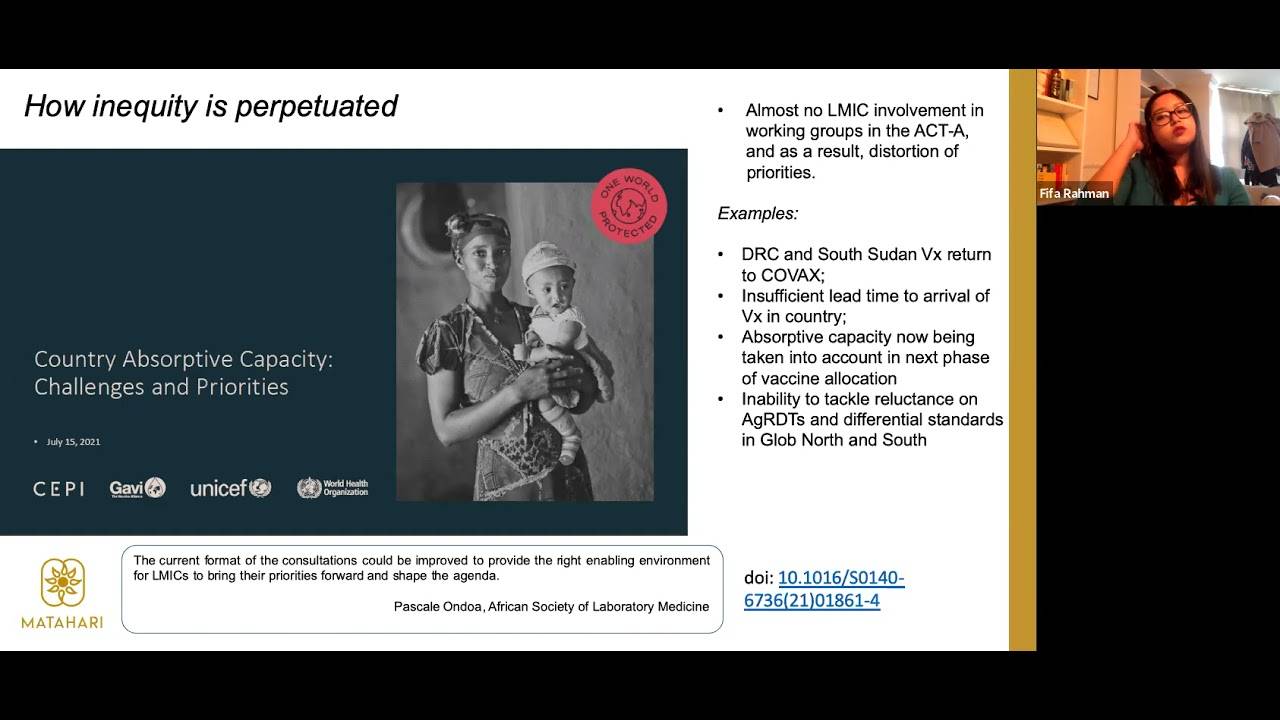
hi everyone we're just gonna wait a couple of a couple of minutes to let people uh join and then we're gonna get started okay so i think we can we can start now and people can still uh trickle in welcome everyone to the health law institute seminar series we have an amazing lineup for uh for this year that are convening our speakers are convening around the theme of health equity and uh beyond recovery my name is adelina i am the associate director of the health law institute here at dalhousie and it is my great pleasure to introduce our first speaker today and to moderate discussion um before i do that there are just a couple of uh housekeeping rules that i would like to share with you uh first of all this uh this uh seminar is recorded uh there won't be the attendees are not going to appear on the video it's just going to be um our guest and myself but you are going to be able to uh rewatch this on the schulich school of law's youtube channel now the other thing is that we do have a closed captioning so if you're not seeing that automatically on your screen uh you have a button a button at the bottom of your screen uh that you can uh you can change to uh turn closed captioning on um the other the other thing is that we have we are using uh the q a box for uh for the discussion today so uh feel free to add your questions in the q a box at any time during our guest presentation and we are going to uh to i'm going to come at the end and put the questions to uh to our guest so without further ado i'm going to introduce our our guest today uh dr fifa rahman who has over 12 years experience working in global health she is a presently a permanent ngo representative on the who access to covid19 tools accelerator representing global ngos in meeting with heads of global health agencies in the global kovi 19 response and in various working groups on kovi 19 country support she was also formerly a board member for ngos at unitade working on equitable access to hiv tb malaria and cervical cancer tools she has been on numerous missions to hiv facilities globally including two early infant diagnosis programs in mozambique hiv self-testing programs in rural areas of zimbabwe dissuasion commission programs in lisbon and needle and syringe programs in scott county indiana at the height of the hiv pandemic epidemic as founder and principal consultant of the global health consultancy matahari global solutions she is currently working on strategy development for tb organizations on mapping access to kovi 19 tools in low and middle income countries and um you know in mapping opportunities in the in the right to health for amnesty international we are very lucky to have dr rahman here today with us and she is going to talk about the lessons in interactivity that kovi 19 has globally created thanks very much for that introduction adelina and i'm looking forward to engaging with you all um i'm just going to share my screen and then we can just get right into it so um first of all i'm going to sort of introduce you to the act accelerator and let you know a little bit about um what my role is and what i do um so this is the structure of the act accelerator and that accelerator obviously stands for the access to covert tools accelerator which you know it holds hosts also the kovacs underneath it you probably know kovacs a lot better than than the other pillars just because it's been such a focus um the kovacs is was designed to deliver vaccines to countries in particular 20 percent of their population should be vaccinated and that was the initial target set but there are other parts of the act accelerator that you should know about there's a diagnostics pillar which i sit on the therapeutics pillar and the health systems connector um and there are several other bodies within the act accelerator um which are important discussion forums the facilitation council is one and i also sit there the facilitation council is hosted at the who it is chaired by south africa and norway and that's usually their ministers of health and it's where the member states sit and um this happens every few months and the member states usually represented by the minister and if not officials close to the minister of the countries in question um present on their priorities their concerns and and what they need um and then there's the principles group which happens every thursday i also sit there and the principal's group is where the heads of the agencies are so that is where um peter sands from the global fund sits that's where dr tedros sits um that's where um whoever who who's the head of an agency um associated with the act accelerator um sits there and of course there are organizations outside the global health like the imf the world bank and other folks that's it then so what might what's my role um in in the three places that i sit the facilitation council the diagnostics pillar and the principles group my role is to basically consult with civil society on all the technologies so i deal with diagnostic therapeutics vaccines and health systems um and basically hold people accountable so you know for example yesterday the us government was present presenting on biden's proposed vaccine summit coming up and um they said something about this this new biden initiative as needing to bolster collective accountability what i did was i basically said um yeah bolstering collective accountability is important but one of the things that civil society will be needing and thinking about as we come to the summit that is occurring in the next two weeks is about usg accountability and that would be as regards deployment of vaccines to the global south so so there are things that i call out and at the facilitation council a member state might say something that i would call out or i would complement and an example of this is when the government of india said we are completely self-sufficient on diagnostics and that was important for me to call out because we know for a fact that um people in india don't have enough access to diagnostics unlike us in the global north where we have these um coveted self-tests at home i don't know what it's like in canada but at least in the uk we can order them free um over the nhs and it comes to your house but of course they don't have this in india so it's important um to to call out those are just two examples of my role in keeping um in your country is and agencies accountable um and and let's go into the detail right so the next slide is talking about how inequity is perpetuated um and this is an important slide to set the tone for this whole presentation as you remember there are there are four pillars of the act accelerator and unfortunately in the working group meetings so under under each pillar under diagnostics there are working groups and and therapeutics working groups vaccines work groups health systems working groups and that's where we work on the nitty gritty stuff right we work on um you know what particular diagnostics are being deployed we work on strategy on these diagnostics we work on and of course there are there are manufacturing working groups in in the vaccines anyways let's spare the detail um but the important point is there's almost no low and middle income country involvement in those working groups and and why does this perpetuate inequity it's because you have the distortion of priorities and i'll give you a couple of examples on why this needs to be improved um and the first example is probably on the drc and south sudan vaccine returned to kovacs so i don't know how many of you know but what happened was vaccines were deployed to democratic republic of congo in south sudan and unfortunately they were unable to deploy this despite vaccine readiness tools completed in in france um those vaccines were sent back to the kovacs which of course takes time effort money to return um so my contention is this and my my theory and and my belief is this is that if we had african experts frequently consulted as frequently consulted as we consult experts in the global north in these discussions this wouldn't have happened right because you have that expertise you could you you have that contact in drc we go if we give you five days notice to send you these vaccines will you be ready to deploy will your community health workers be ready to deploy will your provincial leadership be aware that the vaccines are coming you know do you have the information systems to register people you know all that kind of stuff can be asked to the person if they were included in the working groups right there's also issues with insufficient lead time to arrival of vaccines in country and this was illustrated by a presentation we had from who somalia um this brilliant doctor and he he said that um that there were five days of notice between the deployment and the arrival in country now if you know anything about health systems worldwide is that they vary and one thing that the covid pandemic has taught us is that even the most developed countries in the world like the united states in the united kingdom might mess up on health systems they might mess up on the kobe response and resulting in lots of deaths five days is not enough time for any country um you know especially a country like somalia but despite this they successfully deployed um and consumed 90 of their vaccines and i actually have a slide on this um but i'm telling you now so i'll show you the slide in a second so we can talk about that in more detail another thing is about this new requirement that gavi or the vaccine alliance is using it was using that's a july 15 slide in their next uh deployment of vaccines after july which is assessing country absorptive capacity so if if your country is assessed to have less absorptive capacity you would get less vaccines and i remember the conversations on on the call where this slide was presented and there was a lot of concern from major global health agencies and major global health thinkers that this would be inequitable because just because your absorptive capacity is less does not mean you deserve less vaccines if your absorptive capacity is less there should be efforts integrated immediately to improve that absorptive capacity to reach a certain level and what was promised in the covax was that 20 of populations would be vaccinated so there's obviously real concerns about that um of course the inequity today exists for diagnostics as well and i'm sure therapeutics even though i engage less on therapeutics just because we're still waiting for the therapeutics to come in and come in at affordable prices so obviously i just showed you my um my antigen self-rapid tests which i have in my home and at my work table and i can do them you know every time i decide i want to go out to a bar or a restaurant and um the situation in the global south is very different right we don't you know there's a real inequity in testing because i can do it twice a week if i want and um you know some people are not being tested at all so there's clear problems with with how that works now there's an article there that i've put right at the bottom that sort of illustrates the lack of lmic involvement so pascal and doa is a diagnostics expert she's from the african society of lab medicine and she said in this lancet article and the doi is there i'm not sure if slides will be shared but um look up the article it's by an uh by a journalist called andania usher in the lancet and she said the current format of consultations could be improved to provide the right enabling environment for lmics to bring their priorities forward and shape the agenda so it's really important that pandemic responses going forward because this won't be our last pandemic invest in the equal intellectual partnership of lmics and this is really really important and i'll speak about this further so this is um a slide from last week on the kovacs supply forecast um and i circled there that we're expecting um a further 1.1 billion doses to become available for delivery between september and the end of 2021.
so i did a rough calculation um september to the end of 2021 that is 120 days approximately and 1.1 billion doses divided by 120 days that's about at least 9.5 million doses a day that need to be deployed which is monumental and the question is how exactly is the kovacs going to deploy this you know there are real logistical concerns with um the idea that we're going to be able to deploy these 1.1 billion doses by the end of the year so these are some of the critical questions that we're asking and and you know in in my meeting yesterday and yesterday was thursday so it was the principles group um you know the you know it's it's clear that these things are probably going to stretch into 2022.

so another interesting thing that is coming out of the supply forecast is that gabby is it is changing its tone a little bit and we've of course been demanding sort of transparency increased transparency on delivery schedules because it hasn't been clear to us when say you know pick any country when is haiti going to get their next tranche of vaccines when is somalia going to get the next tranche when is mozambique going to get the next tranche that's not clear to us at all and it's not clear to gavi because what's been happening in the recent meetings with gavi is that they said that they are demanding increased transparency from industry because industry is not being transparent about when the vaccines are coming so overall there is a lot of opacity in in how people are doing things and this is this doesn't bode well for timely a timely pandemic response and this does not bode well for in for equity and we're working every day to try and change this and try and be a voice of accountability so i wanted to address hesitancy because some people have tried to make it an issue um [Music] for lmics and by some people i want to call out the pfizer ceo right who said that even if we made the vaccines available and i'm paraphrasing um there'd be too much hesitancy and they there would be no consumption so this is so problematic on so many levels and of course there's plenty of hesitancy in the united states in in france but there's something underneath that is underlying people's comments about africa and about the developing world on hesitancy and um this article by tian johnson is really worth reading because there is no doubt that there is racism ingrained in what people are saying there is racism ingrained in systems right and to the act accelerators credit um and particularly the diagnostics pillar i think um and the foundation for innovative diagnostics which has been um more engaging with csos and um we've been able to shape their gender more there um they've actually introduced country roundtables where countries are speaking and they can exchange their views and more can be learnt from them there there's also more being done on the principles group by the chair of the principles group which is carl bilt he's a former finance minister of sweden and and you know there's been invitations to lmic experts and and and things like that to try and improve engagement but but it's curious that these things were only done so one year into the pandemic and it happened only this year and the act has been running for one and a half years now so so there are real concerns right so so we've been talking about hesitancy a little bit and you know the fact is it's not so much an issue of hesitancy but more of an issue that the supply isn't there there is inequity in supply and you've i'm sure you've heard the term that people are throwing around around it's vaccine apartheid right and that there's a real problem with the global health architecture as is on covid and not taking advantage of community health workers and their role now of course we could unpack this a lot more but community health workers are largely unsalaried the only global health agency that i know of and and people can correct me if they know of any others but um global fund is probably the only global health agency that salaries community health workers and you know every other agency provides them sort of a travel per diem um for for the work that they do and the community health workers are very important they were very important in the ebola response when they tackled hesitancy there right and i feel like the act accelerator hasn't adequately invested in community health workers now why hasn't this been so what's also needed is sort of a shift in funding right because everyone vaccines is a sexy thing right it's a sexy thing donors are putting all their money into the investment of deployment of vaccines and unfortunately the health systems connector on the act accelerator hasn't sat for weeks months now i think um and community health workers come under them and it's incredibly important that community health workers are funded and of course health systems isn't just about community health workers it's about my apologies i have a parcel apparently but i'll keep talking so um it hasn't sat for weeks and the health systems connector is really about um it's about electricity it's about wash it's about um wash meaning water and sanitation and um all of that it isn't just um community health workers and all these things need to be tackled you know we've got situations like in iraq where the they had a major fire in the hospitals and and um including in the covid wards and a lot of people died and that was caused by an explosive exploding oxygen implements that's a health systems issue right so these are issues that are incredibly important and the fact that the health systems connector isn't funded is a problem now of course why isn't it funded um there are governments in the eu who have given as much as 50 million euros to the health systems connector but we don't know whether money necessarily is has it been rerouted to um vaccines you know there's there's a little bit of of um lack of transparency that we we would like to see further in terms of budgets and things like that to make sure that all the pillars are adequately funded and technologies can be deployed so another question that's important and you know obviously i remember the days when i was doing a master of health law and i was um i was thinking very much about these difficult questions and one of the difficult questions that should be thought about is this issue of who decided that the kovacs would only um vaccinate 20 of populations of these countries 20 20 how you know was it a practical decision in terms of were they thinking okay um rich countries are going to monopolize the market for vaccines so we can only reach 20 percent of lmic's populations you know what was the bar for that and i guess i get i get that you don't want to go okay will vaccinate 800 percent of populations like you know just announce it like that i'm sure there's some rationale behind it but 20 percent isn't enough and 20 is going to create whole populations in the global south that are at risk for um um creating new variants which are of danger to the north right so how does this make sense so these are important questions that need to be um asked this is a slide that i already spoke about in advance but um that i wanted to show you this is the um slide um on the deployment in somalia and 90 of the doses were administered despite having um only five days uh notice but you you would think you know if they had more days how much more could be deployed and somalia is of course a country with a large mobile population um so you know there are concerns also around you know what if people don't have a home what if people are moving um to different areas you know how how are you going to make sure that you administer two doses um but one of the things that was quite clear from this presentation by who somalia was that the the role of the community health workers in reaching out through the communities and bringing elderly people to the vaccination center bringing um mobile populations migrant populations to the vaccination center and the role of the community health workers is incredibly important and this is where health systems overlaps with vaccines the next slide is going to show something quite stark as well so the number of people um who received the vaccine um in a particular age group 5 50 years and above only 23 percent so yeah i'm it's only 23 percent a female were only 18 out of that group right so you know there's a clear disparity um in terms of gender so why are females being less vaccinated and this is this is why it's sort of so important to take an intersectional approach when we're analyzing um any global health issue really especially in vaccine deployment so women often don't they have limited decision-making power on their health they might not own the transport that is necessary to get there um they also are primary uh caretakers of families and and may not have a place to put their children while they get the vaccine there's so many things that affect access to vaccines and gender is quite clearly one of them so um this is this is switching to to um diagnostics and i wanted to show you this because the the iniquity isn't isn't just related to vaccines and i know people are probably raging at this point um about about vaccines but i'll make you rage even further um there have been a number of bottlenecks right in in deployment of rapid tests in particular and rapid tests are important especially when you have vaccine inequity because it helps people control their own risk right and it helps economies stay open um so if you are you're a truck driver um delivering supplies over borders um it would be important for you to have a test done it's important for care home workers is you you probably heard like in the uk so many uh care homes um had so many covert deaths and um my husband works in a in a care home and um he um gets um uh he has we have so many rapid tests just in our home um it's it's it's probably a lesson in inequity in in itself um but he gets tested once a week with pcr and um you know he can test many times a week um with rapid tests so it basically keeps the economies open um it helps people manage risk while while there still is vaccine inequity um so what happened in the act accelerator is there was a diagnostics capacity reservation which sounds fancy but all it means is that um the act accelerator reserved manufacturing capacity volumes of the rapid tests for two companies for supplier under that accelerator so they booked the manufacturing space basically um as time progressed it became quite clear that countries weren't taking up the diagnostics as quickly as they should right it was quite low demand for the rapid tests and everybody was like why so what happened was they commissioned a study to look at bottlenecks um you know what are the key bottlenecks what what um what are the issues why why are countries not asking the act accelerator for rapid tests so there are a number of um uh reasons um that countries gave which are um listed there on your screen but one of the things that i kept hearing because my job is to outreach to people in country and ask what's going on and one of the things we kept hearing is that wkho guidelines are too restrictive it doesn't allow us to use the tests for what we want to use them so this is interesting because this was who being about bottleneck right so what we did was we had a look at the um the guidelines and i'll tell you that about that in a minute but what was clear was that we needed decentralized decentralization of testing and these are some of the things that countries said right so um [Music] a kenyan guide interim guide for antigen rapid diagnostic tests said only qualified registered and licensed medical laboratory officers can carry out the tests so community health workers would be able to to to use these tests right i mean these are really easy to use they mean just follow the instructions you can do it yourself you can report it at least in the uk to the nhs whether it's negative or positive through your through your phone and of course there are questions about the digital divide and what about people living in poverty and not being able to report it but anyone can do these tests they're not very hard to do um so the fact that some countries had quite conservative interpretations of who could and still can you know a lot of countries still have conservative approaches to antigen rapid tests is a real impediment for making sure there is empowerment on testing in the global south so there's covert 19 testing in south africa and that should be conducted in authorized labs only samples to be collected by trained healthcare workers now this language is a little bit better just because um there's some room for interpretation right um if you're trained to deploy it and if you're a community health worker you could potentially do it right um but it has to be conducted on site rather than at home which is you know you know what we want is for tests to be able to be done in communities especially for marginalized communities people who use drugs internally displaced people all all these kind of people you know they need it's better for these tests to come to them in their communities and a key challenge there is that the community health workers aren't empowered to do this so um that's obviously a real problem this is the letter that i signed and wrote to the wh show about my concerns with the testing guidelines that they were too restricted to certain use cases and use cases is just the word to say you know where they're being used right um and we were concerned about the inequity resulting from this um and this of course went to dr tedras maria van kerkov and dr sumiya who's the chief scientist of the world health organization um and of course this letter uh went to them after a principles group call where i was i was raging about it really i was just like this is really problematic who's guidelines are a bottleneck and um we were of course really quite concerned and one of the things that was said to us was like if you interpret the guidelines you can you can use these tests in communities and my problem with that is that if you need creative interpretation to do something in your country the guidelines are not good enough right so that was the concern and this was quite a long letter you can read it if you like or use it for your essays and dissertations or lectures um but as you can see the date on that is 9th june but this resulted in a lot of discussion on 16th june and i'm just letting my cat out on 16th june um the who issued these infographics so um [Music] the infographics are um important because we've been making so much noise on communities um living we wanted the test to get to communities and if you look at these infographics and we've also in the letter we demanded we wanted to see um um visual um tools right sorry this is this is i expected this and i told edlina that this might happen um so um as you can see it says there that um they are looking at communities where there is ongoing transmission so um our letter was on 9th june this happened on 16th june so um it's quite clear that um our work is is resulting in something right um i i don't think this language is clear enough but it's a step in the right direction so um it's really quite important to keep going on this work and to make sure we have testing everywhere um the next thing i want to talk about is oxygen now we all know about the oxygen crisis that happened in india and the deaths that occurred from that but there are oxygen crises happening every day in multiple countries uh now this is a very busy graphic um obviously um but as you can see the countries where which are displayed in red um have high and rising oxygen need so you've got india um iran um they've got serbia um mongolia you've got costa rica palestine ukraine um there are lots and lots of countries that are struggling with with with high oxygen needs so um there's a lot of oxygen inequity as well um and what are lessons from this uh because i am supposed to talk about lessons and not just be a series of complaints or concerns um the the top um oxygen companies in the world they're they're all based in the global north so there's six of them that includes air lender and and a number of other um oxygen um producers and um there are real opportunities for building more facilities in the global south because there are gas companies in the global south um who are producing nitrogen and things like that for industrial use and oxygen is really a byproduct so the question is how do we decolonize and decentralize and make sure that countries in the global south um um have a manufacturing capacity there's a lot that needs to be done on supply chain and health systems issues and to make sure that this improves for the next pandemic but as you can see it continues to be a major problem um across the world i wanted to go to therapeutics as well um and um monopyravir is um it's it's there's a lot of buzz around how um how brilliant it is um and sometimes this buzz didn't turn out there's a lot of buzz earlier about gileads rem de severe but that turned out to be just incorrect and and we don't use rem december today for um covet but there's a lot of basel on multnoperavir because it can be used um as an outpatient treatment and what does that mean that means um someone gets diagnosed with covid um potentially at home right if they have rapid self-tests they can do that at home and um [Music] they could i don't know in a health system have um a doctor come to their home and deliver the monopoly to them reducing the risk of them spreading um covert to others and infecting others and they could be treated within the home so it's exciting right um and this is where health law comes in in the intersection of intellectual property so there were voluntary licensing agreements with five generic indian generics manufacturers to accelerate the access to modern peer review and um it's you know there's a lot there was a lot of critique coming out of this because now i can't remember how many countries allowed it to supply it to but it was i think 105 countries or something like that um who would get access to the generic monoperview but there are more than 105 countries in the world um who chooses these countries um are countries like russia included probably not countries like china included where there's a massive poverty problem um included um uh middle-income countries included you know there's a lot of questions about um equity which is really what this presentation is about um and there's a lot of questions on whether compulsory licensing would be better so what is the difference right a voluntary voluntary licensing is basically where the company voluntarily does it right and compulsory licensing is where usually the country the country who wants the cheaper generic medicines has to negotiate with the company um to say okay are you able to give us a cheaper price right and if the country country the company goes no we can't give you a cheaper price um then the the the country can override the patent and they can issue a compulsory license and depends on which country whichever ministry does it in malaysia for example it's a trade ministry that issues compulsory license and what happens is um you know it overrides the patent which allows the generic manufacturer to manufacture them at a cheaper price so a lot of people were saying are compulsory licenses better for this kind of situation um and it depends i mean i'm all for compulsory licensing i think a lot of these things are publicly funded with our tax dollars and pounds and um and and whatever currency um it is and you know should there be a reckoning um and a return on investment um to the people right because people are putting the tax dollars into this um should should these be so that the prices they sold at so that's that's one of the things um that are that is obviously of concern and i want to go to health systems um now and obviously i've talked about health systems throughout because health systems is so linked to every one of the issues that we've discussed so far now i told you earlier that the health systems connector which is one of the pillars in the act accelerator has not sat for weeks or months right and health systems connector in the start of the act accelerator last year when we had the pandemic uh the start of the pandemic if you look at what this article says um the act accelerator focused on medical oxygen and ppe which are components of clinical care they're not really health systems and this year we saw oxygen move to the therapeutics pillar which is you know it is a treatment it's it's one of the most effective treatments for covid and um it belongs in this in the therapeutics pillar that left ppe within health systems but health systems isn't just that i i told you this before health systems is making sure community health workers are out there in the communities bringing people to get vaccinated um you know participating in health education telling people about the risks of certain things bringing tests to people right so community health workers is a major thing that wasn't addressed then but um we know that the health system is connected today while it hasn't sat for some time is doing rapid assessments on what countries need so this is a start but it needs to be i know they're rapid assessments but it needs to be quicker because health systems are falling apart and it's really important that they are sorted or strengthened um it's it's a big task but it needs to be done so one of the things that we're asking for is more transparency in the health systems connector and um you know it's it it's incredibly important because what what have you got you've got on the screen right now is a matrix from july 2020 and i told you about the working groups that happen in the health systems connector and i know there's a lot of technicality in it but this was the community-led responses um work stream and there's several priorities in there there's the need to improve basic infrastructure at um public health facilities including wash which is water and sanitation um and hygiene electricity connectivity um scale up of training for frontline services availability of ppe so this is just some i only took a tiny snapshot of what the priorities were in july 12 2020 where it's september 2021 and i don't know and i i'm my job is to know a little bit about everything right to this date i don't know the progress on any of these deliverables and i'm having conversations with these people all the time so what happened to this matrix why have we not strengthened health systems in a way where they're supposed to um you know it's it's a real problem and i get the whole argument that this is our first rodeo right this is our first rodeo we're gonna mess up but but we also need to ask questions and keep people accountable and this is one of the key questions right what happened in health systems now there's some um and i keep emphasizing community health workers because it's so essential and this is such a good article to read because um madeline ballard did this time series analysis and she found that community health workers who equipped and prepared for the pandemic were able to maintain speed and coverage of community delivered care during pandemic period she also points out that committee health workers globally remain unpaid and unsupported which i mentioned before and the paper that suggests that the opportunity costs of not professionalizing community health workers may be larger than previously estimated so there's a major gap in the fact that we don't invest in community health workers and this is one of my final slides i think um and i'm not sure where i am on time um that's an hour um um but but important to end here this is a slide from yesterday um it shows that to deploy the amount of doses we need to deploy um by the end of 2021 um health systems have to be four times um stronger right um and how can that be done i mean it says on the right um field there health systems must be must be ready to deploy more doses than accustomed to in the past which is nice to say right it's it's a it's a nice aspiration it's an important aspiration but how do we do that when health systems aren't adequately funded um [Music] it's important and there's no kind of road map on health systems um in the code response and it's concerning so final slide um is that there is an act accelerated strategic review ongoing um and i've been interviewed for it um and um it should be out soon um one of the things uh that i was concerned about and the question that i got by the consultants was what kind of structure do we need to consult along ics which i think is so loaded and problematic because we don't really have a problem consulting white global north experts we just email them there's this thing called email it's miraculous we don't have problems going to this professor at boston university hey what you know i'm concerned about xyz what you know what can you tell me about this we need to do that fella my sees i i don't know why we're not doing that and peop you know people think like oh to consult lmic's you need some kind of special structure some kind of integrated structure which is great i mean if you want to do that do that but you know it shouldn't be in a tokenistic kind of way you know it shouldn't be the way i foresee it it's as if that structure is reserved for the comments of lmic's and it happens once a month or or wherever when you should you should be consulting regularly and if there's a problem in drc you should have that expert in drc ready in your whatsapp to go hey um i'm concerned about this you know do you think community health workers are ready do you think you know how many days do you need to get the vaccines what's the situation with your rapid tests right um which leads to the larger question of um the fact that we need to decolonize global health architecture and we need to um quite clearly make some basic statements to people running things right um you know why why didn't you consult a drc expert why didn't you consult somebody in south sudan why didn't you do that um so there are real problems with global health architecture that need to be tackled and and they make they're uncomfortable questions they make they make some people quite constipated especially when we say things like racism or you know it but it it's important to mention because it distorts priority uh a pandemic response for the future needs the equal intellectual partnership of lmic it needs that indigenous knowledge and until we learn how to do that until we learn how to make friends in the global south and and send those emails and and and not feel the need for any specific structure all those structures are important as well we're not going to be as effective as we would like thanks and i'm happy to to get questions thank you so much fifa for that amazing presentation um i would like to encourage people to use the q a box now uh to uh to ask questions um we already have a couple of questions here they are from matt herder who's the director of our health law institute here so i am going to um i'm going to read out the question just so everybody can hear it um uh dr raghman you can you can see the questions as well in the q a if you if you need a visual um so matt says thanks for uh for a wonderful thought-provoking presentation it really helped me to understand how the accelerator operates my question is about this governance you noted the example of the fighter ceo making problematic claims about vaccine hesitancy in africa industry is represented within the accelerator what happens when industry representative representatives make such comments which others engaged in the accelerator likely disagreed with did that slow the work of the accelerator did it fragment it how are tensions among the different actors with conflicting interest mediated more broadly i'm curious about your reflections on how to improve the governance of pandemic responses in the future given the division between public and private actors in the global north and the global south so um these are such important questions um so industry has multiple times so industry is in the principles group as well um and um [Music] there was actually a moment where and it was brilliant and and i i have so much faith in the wh odg and i know you know there's been some horrifying articles out there about his competence and his links to china and all sorts of crazy things um [Music] but this was about um making sure manufacturing of vaccines could occur in the global south and um thomas cooney who is the um from the international federation pharmaceutical manufacturers said the language was not appealing to industry um something along those lines um and dr chadros made an impassioned speech for equity um and it was it was very important um for him to say that there are things like that um but your question was on how to improve governance it's a lot of things it's i mean industry has its uses right i mean they are the ones producing the vaccines um but at the same time you know governance needs to be improved so much and for example the vaccines pillar didn't have csos uh till much later um all the other pillars had civil society much earlier um and the answer in the global south and the global north that that unfortunately requires us to engage with with questions that make us uncomfortable um and i know michelle bachelet she said we need to tackle systemic racism to uproot it and that's it racism and it's it's funny how many people just recoil at this word they're okay with diversity and inclusion but they're not okay with the word racism and it really needs to be sorted because it's endemic in global health um and governance structure wise um it's it's um [Music] it's hard to say because in in in the actor there isn't just one decision-making um pla place you know it happens across multiple um working groups it happens behind the scenes it happens at the facilitation council that happens at the principals group they happen everywhere and maybe some kind of specification as to where decisions are made would help thank you um we have another question um so thinking about the periods in between pandemics and epidemics what are the policy levels and strategies that might help to ensure equitable access of infectious disease interventions and then there is an explanation here um in asking this question i'm thinking about how universities and other public research institutions have let us down the lipid delivery system that is integral to fighter and modern vaccines came out of the university of british columbia and ubc's tech transfer office has been lauded for having strong principles of global access yet none of those principles seem to have been applied to ensure that the delivery system could be licensed out to entities in the global south so if universities won't follow through at least not voluntarily what other strategies and policy levels might be deployed instead i think it's a really good question and i'm thinking immediately of the whole transparency resolution um and how we need more discourse and how the global health architecture is broken and how the voluntary system doesn't work because we had this wondrous um transparency resolution well not wondrous because i know a lot of things were deleted from it um but in the end it said that that countries would commit to being more transparent about the the costs of r d the origins of r d into into uh global medical tools and and you know like and and to to relate the cost to to to that right um so but you know what what has been the progress on the transparency resolution what accountability mechanisms has been on has has occurred on that we don't know if you know which countries have been more transparent with with you know where you know where these tools came from and you know whatever is in the transparency resolution needs to be applied to universities as well like what what did you contribute to this you know how much of your money is publicly funded um you know why what's the recipe right and one of the things that we're thinking about is um you know what there should be is a whistleblower blowing line either hosted by you know maybe human rights organizations could host the whistleblowing online for for people within universities that develop these things or you know within companies even so so if there's a a fisa scientist who wants to come out and call the whistleblowing line and say i have this a bit of recipe uh of the vaccine or things like that that that's that's another thing that that we need to use creative ways to get to these things just because um they're just not going to to happen with voluntary mechanisms okay so another question um advanced market commitments the tool used by kovacs to get vaccines from sponsors has been found inappropriate by some scholars mainly because it puts kovacs into competition with deep pocketed high-income countries what has been your experience or observation with the advanced market commitments thanks so much for this question and it's um it's a it's a it's a real problematic one because um one of the things that we've been concerned about is the uk of course dipping into the doses with covax and i've you know i've just been really these are global south need the doses and the uk and and i live in the uk and and we have at least four or more like some articles say seven four nine we have at least four or more doses per person so the uk has completely overbought and and monopolized the market um and yet they got doses from from kovacs now gabby's response has been to this has been that they need to honor their agreements um it's it's of course problematic you're correct um and and now we know better but the the good thing is i suppose is that um a lot of the countries who have overbought vaccines they have enough vaccines for their countries are now saying we don't want um the allocation that was provided to us um under the kovacs so that's good but it's voluntary there's no way to compel them to say no to their covax doses you know and there are countries like the uk who will keep saying yes um and this is obviously digging into the supply from the global south so definitely problematic do i have an answer to how to solve it for the next pandemic to not allow it but for now what do we do um welcome to your suggestions okay so we have time for one more question i'm just going to and we're going to end here because i think that's a that's a question that a lot of people have um and it's about the boosters do folks within the accelerator worry about the impact of boosters on the global vaccine supply any counter strategies apart from the important statements that dr tedros and other global health advocates have already made counter strategies you know it's it's something that i'm sure my colleagues in the vaccines pillar are thinking about right now our latest update is that the you know folks in the who are not going to issue any recommendations on them at this stage there is some evidence that um that they are beneficial for immunocompromised people um you know that could be elderly people or people um cancer survivors and and things like that which is like okay fine but it's clearly going to dig into to markets when most countries haven't even been vaccinated by one percent it's so problematic and strategies tough question maybe maybe matthew you and i need to sit down and strategize together on how to um how to how to solve these problems um but it's it's a big question and and question i don't actually have the answer to but but it's an important one and we need to um try to figure out but you know vaccine manufacturing in the global south is clearly clearly something that we need to to think about um it's it's the whole global health architecture and i know it sounds like a broken record but it is heavily broken and um it's sort of pandemic profiteering we're seeing is is insane so um more conversations to be had to get the answer the answers um thank you so very much you have some some uh some thank yous in the in the chat as well from people i think uh uh your talk was really well received and we're very grateful for you for uh taking the time uh to join us today for our uh for our seminar in this very important conversation um and as i said the uh the the recording will be available on the youtube video for those who want to rewatch or share um and our next uh our next seminar is going to be october 8th with the dr holly northam of university of canberra talking about um restorative approaches to remove institutional and professional barriers to uh human flourishing also is going to be um online via zoom uh thank you again so much dr rachman and uh thank you for sharing uh your knowledge and for the important work that you are doing my pleasure and thanks so much for having me thank you